COVID-19 Update May 15, 2020 from Rabbi Aaron E. Glatt, MD
With last week’s release of both the OU/RCA and Agudah guidelines, there has been much debate within the local and national Jewish world about what will now happen. Practically, not much has really changed as the official state statute still prohibits religious gatherings:
Pursuant to Executive Order 202.10 , all non-essential gatherings of individuals of any size for any reasons (e.g. worship services, parties, celebrations, or other social events) are canceled or postponed.
Further, individuals should not gather in houses of worship, homes, or other locations for religious services until the end of this public health emergency. If possible, religious leaders should consider alternative forms of worship, replacing in-person gatherings with virtual services, such as phone or conference calls, video conference calls, or online streaming.
In other words, the Governor has to first permit us to return to any sort of public religious life (minyanim, weddings, levayos, etc.) as well as educational life (schools and camps) before our rabbonim can decide what is halachically allowable. In the words of a great talmid chocham – we can be more machmir than the governor, but not more meikal. More to come about that at our 9:30 PM Motzei Shabbos Zoom conference.
What have we learned in the past week about the virus and immunity?
A lot! An excellent summary from the CDC published in JAMA stated that viral “burden” (the amount of contagious virus) typically peaks early in illness, and declines as antibodies develop. Antibody titers rise over the subsequent 2 to 3 weeks and then level off. Virus declines quickly during the first week of illness, however the absolute duration that a patient might shed infectious virus is unknown – but is probably not much beyond 7-10 days. Persistent detection of viral RNA weeks after recovery from COVID-19 does NOT represent a meaningful clinical or public health risk, especially in the absence of symptoms. Indeed this is one of the most common questions people ask me – am I still contagious. The NYC Department of Health just declared that COVID-19 positive patients (except those severely immunocompromised) who are feeling better, are at least 14 days from symptom onset, and have no fevers for at least three days, are considered non-contagious. And this is even if they are tested and still have a positive COVID-19 swab test! Therefore, there is NO NEED to get repeat tests.
Most importantly, to date, no human reinfections with COVID-19 have been confirmed. Plus, there is also no evidence at present that such persons transmitted COVID-19 to others after they had clinically recovered. However, this possibility of transmission cannot be ruled out, especially for persons who may be predisposed to prolonged shedding due to immunocompromised states.
Finally, existing limited data on antibody responses to COVID-19 and related coronaviruses, as well as one small animal model study, suggest that recovery from COVID-19 might confer immunity against reinfection, at least temporarily. The durability of neutralizing antibodies (antibodies that seem to provide immunity) against COVID-19 has yet to be defined; persistence up to 40 days from symptom onset has been described. However, the immune response to COVID-19 is not yet fully understood and definitive data on immunity are lacking.
Bottom Line: We are learning more every day, and our understanding of immunity to COVID-19 is beginning to materialize. But we all must still socially distance for the time being.
What have we learned in the past week about the disease?
Three new findings of interest to discuss here. The above section was quite technical. But low tech works very well too!
1) A just published paper in Nature Medicine showed that loss of sense of smell and taste were among the most reliable early screening findings to identify COVID-19. Among more than 18,000 participants using a smartphone-based app to report COVID-19 symptoms in the U.K. and the U.S., about two thirds who tested positive for COVID-19 had as one of their first symptoms (and sometimes the only symptom) loss of taste and / or smell.
They concluded: “This could be used as a screening tool to help identify people with potential mild cases who could be recommended to self-isolate”. We have been recommending this since early in the pandemic, and now we have solid proof that this is a very smart epidemiologic and public health SIMPLE method of preventing spread of COVID-19. Maybe, in addition to checking temperatures before going back to work, we should give everyone a rose and only those who pass the sniff test get to enter.
2) In a cohort of 1,590 patients in China published in JAMA, a predictive model of severe disease was proven in a validation cohort of 710 patients. What does that gibberish mean? Well, they looked at 72 potential variables, and determined that 10 parameters were indeed independently predictive and could be put into a simple statistically valid scoring system to calculate who will have a better or worse prognosis. Included in the risk score were personal data, symptoms, lab values and x-ray findings.
The score has been translated into an online risk calculator that is freely available to the public by clicking here . An easy tool for physicians to use and help guide treatment to COVID-19 patients and their families at the time of admission.
3) What is known about how COVID-19 is spread? “Superspreading” events
involving COVID-19, have been reported. One only has to think about how fast the virus spread within some families and some neighborhoods to appreciate the importance of certain activities / gatherings in promoting illness.
An elegant paper in the MMWR discussed one specific choir practice (think communal shul singing and chazzanus) and the subsequent spread of COVID-19 there, demonstrating the serious potential for spread in tightly packed indoor public gatherings.
Following a 2.5-hour choir practice attended by 61 persons, including a symptomatic index patient, 32 confirmed and 20 probable secondary COVID-19 cases occurred (attack rate = 53.3% to 86.7%); three patients were hospitalized, and two died. Transmission was likely facilitated by very close proximity (within 6 feet) during practice and augmented by the act of singing.
The potential for superspreader events underscores the importance of physical distancing, including avoiding gathering in large groups, to control spread of COVID-19. Enhancing community awareness can encourage symptomatic persons and contacts of ill persons to isolate or self-quarantine to prevent ongoing transmission. Very scary indeed.
When will the Governor loosen restrictions and open businesses?
The governor is expected to open up 4 upstate regions in NY today, but none of the downstate regions have met his preconditions for easing restrictions at this time.
To follow these criteria yourself, go to the following websites:
The Regional Monitoring Dashboard can be accessed by clicking here
The Daily Hospitalization Summary by Region can be accessed by clicking here
What have we learned in the past week about treatment?
Also, a lot! Four important studies demonstrated efficacy using four different treatment regimens.
1) In a retrospective cohort study of COVID-19 patients with severe lung disease (but not on a ventilator), treatment with high-dose anakinra, an interleukin-1 inhibitor, was safe and associated with clinical improvement in 72% of patients. Confirmation of efficacy will require controlled trials.
2) Treatment with interferons may significantly improve virus clearance and reduce levels of inflammatory proteins in COVID-19 patients, according to a new study in Frontiers in Immunology.
Researchers in Wuhan found that treatment with interferon (IFN)-α2b significantly reduced the du-ration of detectable virus in the upper respiratory tract and reduced blood levels of interleukin-6 and C-reactive protein, two inflammatory proteins found in the human body. Such inflammation is assumed to cause many of the complications of COVID-19 illness.
3) A three drug combination – kaletra (a well-known HIV medication), ribavirin and interferon – was shown to improve outcome in patients with milder COVID-19 disease. Kaletra alone has not been shown to be effective but in combination it may be another useful modality.
4) The first US data on plasma therapy were published and are promising. The safety profile of plasma was excellent, and it appeared beneficial in a small group of patients in Texas. Our own plasma experience is now at 100 patients, and we will be completing our analysis in the near future.
How do you think COVID-19 will end?
I was asked this question by a national ID news magazine and this was the answer I supplied.
“It is impossible to predict with any accuracy when we will see the end of this horrific COVID-19 pandemic. I will go out on a limb and provide predictions for the U.S. and globally.
We currently are fighting a lethal enemy with our hands tied behind our backs. Without a vaccine, or a safe, oral, effective treatment; and with still insufficient easily available noninvasive rapid testing; the only tool we have to control COVID-19 is social distancing.
While social distancing is an effective tool, it comes with a very high price tag – essentially uprooting society as we knew it.
Social distancing is causing spiritual and economic upheaval (that has not peaked yet); massive unemployment; delaying non-emergency medical care and disease screening; and is disrupting our educational system. In short – it has very negatively impacted people’s lives.
At this point in time, we are struggling to even control spread of disease with these draconian distancing measures. I do not think society as we know it can continue in this fashion for a long period of time.
Ultimately, I believe technology will be the only solution besides prayer. My hope is that a efficacious and safe vaccine will be developed for use in early 2021, which will be our best chance for bringing COVID-19 to its knees. Short of that, we will be constantly counterpunching with only moderate success.”
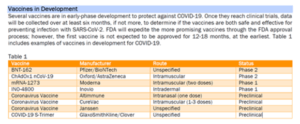
Below is a table put out by Express Scripts updating where we stand today with vaccine development. Human trials have begun and over 70 companies are competing at warp speed for a successful shot. Whether it will take 12-18 months or half that time remains unknown. Be’ezras Hashem it will work.